Paul McMaster is a 30 year old delivery van driver who overbalanced at work whilst loading parcels into his van. He sustained an inversion sprain of the left ankle 3 days ago and has a severe sprain to the lateral ligament complex of the ankle. At present it is difficult to diagnose precisely as the ankle is very swollen/bruised and painful on certain movements and he requires crutches to walk. There is No Bony Injury to the ankle, but he is keen to return to activities as soon as possible. He has a pronounced limp and in not weight bearing evenly through the ankle, showing obvious pain as a result. He lives with his girlfriend in a 2nd storey flat.Subjective assessment
30 year old maleDiagnosed with inversion sprain Pain when weight bearing on injured leg and requires crutches. PMH - NilDH - NilSH - Working as a delivery man, keen to return to activities as soon as possible.Lives with girlfriend in a 2nd strey flat.
History of present condition:
· 3 days ago-overbalanced at work while loading parcels into van.
· Twisted weight-bearing plantarflexed foot sustaining an iversion sprain to left ankle.
· No breakage or fracture.
Expected Signs & symptoms:
Severe sprain-
· Complete tear to muscle.
· significant muscle weakness and severe loss of function.
· Severe pain followed by no pain.
· Minimum to no pain on isometric contraction.
· Bruising (ecchymosis), swelling, and tenderness
· Gross joint instability.
· Pronounced limp in left foot during left stance of gait cycle,weight bearing causing obvious pain.
· Inversion and planatarflexion aggravate condition.
· Possible haemarthrosis
Objective Assessment: tests to determine if there is any abnormal motion at the joint which would indicate how badly a ligament has been torn.
Active movements:
Plantarflexion – 0-15
Dorsiflexion – 0-55
Inversion – 0-20
Eversion – 0-10
Passive movements(assissted):
Plantarflexion
Dorsiflexion
Inversion
Eversion
Special Tests:
Anterior drawer sign:-
Tests lateral ligament and medial ligament integrity.
Patient prone with knee flexed.
Apply posteroanterior force to talus with ankle in dorsiflexion and then plantarflexion.
Expected signs- excessive anterior movement(both ligaments affected) or movement on both side only(ligament on that side afffected)
Talar tilt:-
Tests –in adduction tests mainly the integrity of calcaneofibular ligament but also anterior talofibular ligament.
-in abduction tests integrity of deltoid ligament.
Patient lying prone,supine or on side with knee flexed.
Tilt talus into abduction and adduction with patients foot in neutral.
Positive sign- excessive movement.
Thompsons test:-
Tests Achilles tendon rupture.
Patient lying in prone position with feet over edge of plinth.
Squeeze calf muscle.
Positive sign-absence of plantarflexion.
Gait analysis:-
Pronounced limp in left foot during left stance of gait cycle,weight bearing causing obvious pain.
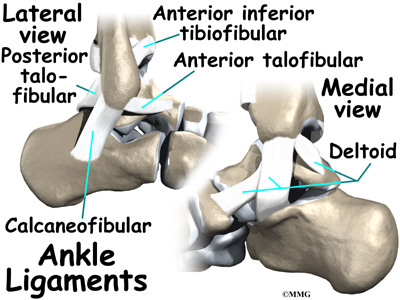
Basic anatomy of ligaments in ankle
Three ligaments make up the lateral ligament complex on the side of the ankle farthest from the other ankle. (Lateral means further away from the center of the body.) These include the anterior talofibular ligament (ATFL), the calcaneofibular ligament(CFL), and the posterior talofibular ligament (PTFL). A thick ligament, called the deltoid ligament, supports the medial ankle (the side closest to your other ankle).
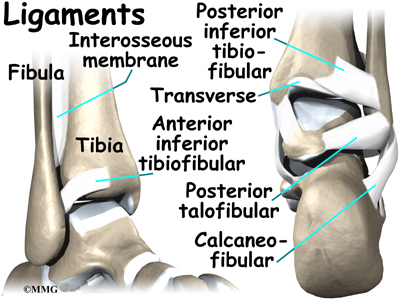
Ligaments also support the lower end of the leg where it forms a hinge for the ankle. This series of ligaments supports the ankle syndesmosis, the part of the ankle where the bottom end of the fibula meets the tibia.
Three main ligaments support this area.
The thin, flat ligament crossing just above the front of the ankle and connecting the tibia to the fibula is called the anterior inferior tibiofibular ligament (AITFL).From tip of fibula to lateral talar neck.
The posterior fibular ligaments attach across the back of the tibia and fibula. These ligaments include the posterior inferior tibiofibular ligament (PITFL) and the transverse ligament. The interosseous ligament lies between the tibia and fibula. (Interosseous means between bones.) The interosseus ligament is a long sheet of connective tissue that connects the entire length of the tibia and fibula, from the knee to the ankle.Short lig. posteriorly fibula-talus.
CFL –cord like structure directed inferiorly and posteriorly to calcaneus.
ATFL most comonly injured,inversion during plantarflexion is main cause of sprain.
In plantarflexion ATFL is under tension and susceptible to injury.CFL may also be injured.
Onset of P important and ability to weight bear immediately after injury.
Uneven terrain , previous injury, badly fitted shoes.
What is an ankle sprain?
An ankle sprain occurs when there is a stretch or tear in one or more of the ankle ligaments and/or soft tissue of a joint caused by sudden adduction . Ankle ligaments are slightly elastic, fibrous bands of tissue that keep the anklebones in place.
Depending on the severity of the injury, an ankle sprain is classified as follows:
· Grade I - Pain is present(mild), but there is minimal ligament damage and minimal loss of function. Mild stretch ATFL, stretch to partial tear of ligament
· Grade II - There is moderate ligament damage and moderate pain ,with a somewhat loose ankle joint.Complete rupture of ATFL without CF invlovement and other sprains with partial tearing of both.
· Grade III - One or more ligaments is completely torn, and the ankle joint is very loose or unstable. Loss of function and severe swelling.
A third –degree sprain of the lateral ankle,which usually occurs as a result of severe inversion injury, causes a complete tear or rupture of the anterior talofibular (ATF) ligament, often the calcaneofibular (CF) ligament, and occasionally the posterior tibiofibular (PTF) ligament. When the ATF and CF ligaments are both torn and subtalar joints. The ATF ligament is most likely to tear when forceful inversion occurs while the ankle is plantarflexed. Associated injuries that occur include a transverse fracture of the lateral malleollus or an avulsion fracture of the base of the 5th metatarsal (both have been ruled out in this case study).
85% of ankle sprains are inversion sprains.This is due to the fibula extending further than the tibia.this length difference results in more eversion vs the tibia.
Deltoid complex is much stronger than the lateral ligament complex of ATFL,PTFL and CF.
In addition to significant pain,swelling and tenderness, a complete tear of one or more lateral ligaments causes a marked mechanical instability and functional instability of the ankle during weight bearing activities. This generally requires crutches.
Mechanical instability is defined as ankle mobility beyond the physiological ROM, increased talar tilt, and an anterior drawer sign. Functional instability is characterized by the sensation of the ankle “giving way” experienced by the patient. As many as 20% of pts without evidence of mechanical instability complain of their ankle giving way after severe lateral ankle sprain, thus significantly impairing functional activities.
After acute, grade 3 inversion injury, nonoperative treatment is successful for most patients. However some patients sustain recurrent inversion injuries after the acute injury has healed and develop chronic, symptomatic instability. For patients with demonstrated mechanical instability who do not respond to nonoperative management and for selected patients with acute lateral ankle injuries who regularly engage in high impact activities, surgical repair or reconstruction may be required to manage the instability and return the patient to the desired level of function.
Goals of surgery and postoperative management is to restore joint stability while pain free, functional ROM of the ankle and the subtalar joints.
Indications of surgeryà
Frequently cited indication for surgical repair of the soft tissue of the lateral aspect of the ankle
Chronic mechanical and functional instability of the ankle during activity,which remains unresolved after conservative management.
Acute, third degree lateral ankle sprain resulting in a complete tear of the ATF and/or CF ligaments.
What is Acute Inflammation? Inflammation is the body’s normal protective response to an injury, irritation, or surgery. This natural “defense” process brings increased blood flow to the area, resulting in an accumulation of fluid. As the body mounts this protective response, the symptoms of inflammation develop. These include:
Swelling
Pain
Increased warmth and redness of the skin
Inflammation can be acute or chronic. When it is acute, it occurs as an immediate response to trauma (an injury or surgery)—usually within two hours. When it is chronic, the inflammation reflects an ongoing response to a longer-term medical condition, such as arthritis.
Inflammation is not the same as infection. Infections are caused by bacteria, fungus, and viruses, and infections sometimes produce inflammation. However, infection and inflammation are treated very differently. Your foot and ankle surgeon can best determine the cause of your inflamed tissue.
Treatment To reduce inflammation and the resulting swelling and pain, injured tissue needs to be properly treated. The earlier you start treatment, the better.
Treatment for acute inflammation consists of “RICE” therapy—which stands for Rest, Ice, Compression, and Elevation. For acute inflammation in the foot or ankle, your foot and ankle surgeon will recommend "RICE" therapy.
Rest. Stay off of your foot as much as possible to prevent further injury. In some cases, complete immobilization may be required. Your doctor will decide whether you will need
crutches and whether movement of your foot or ankle is appropriate.
Ice. Icing, which decreases blood flow to the tissue, thus reducing swelling and pain, should be continued until your symptoms resolve. Wrap ice cubes—or a bag of frozen peas or corn—in a thin towel and place the pack on the injured area for 20 minutes of each hour you’re awake. If your skin turns blue or white, discontinue icing for a few hours. Two cautions: Never apply ice or frozen bags directly to your skin. And never leave an ice pack on your injury while you sleep.
Compression. Keep the inflamed area compressed by wrapping it in an elastic bandage or stocking. Compression prevents additional fluid accumulation and helps reduce pain. Wrap the bandage more firmly at the toes and less firmly at the calf. If your toes tingle or your foot throbs, the wrapping may need to be loosened. If the tingling or throbbing continues after loosening the wrap, contact your doctor as soon as possible.
Elevation. Keeping the foot elevated reduces the swelling by allowing excess fluid to drain to the heart. The proper way to elevate your foot is to keep it level with or slightly above the heart. Place one or two pillows under your calf, and make sure your hip and knee are slightly bent. Never keep your leg extended straight out.
What is Acute Inflammation? Inflammation is the body’s normal protective response to an injury, irritation, or surgery. This natural “defense” process brings increased blood flow to the area, resulting in an accumulation of fluid. As the body mounts this protective response, the symptoms of inflammation develop. These include:
Swelling
Pain
Increased warmth and redness of the skin
Inflammation can be acute or chronic. When it is acute, it occurs as an immediate response to trauma (an injury or surgery)—usually within two hours. When it is chronic, the inflammation reflects an ongoing response to a longer-term medical condition, such as arthritis.
Inflammation is not the same as infection. Infections are caused by bacteria, fungus, and viruses, and infections sometimes produce inflammation. However, infection and inflammation are treated very differently. Your foot and ankle surgeon can best determine the cause of your inflamed tissue.
Treatment To reduce inflammation and the resulting swelling and pain, injured tissue needs to be properly treated. The earlier you start treatment, the better.
Treatment for acute inflammation consists of “RICE” therapy—which stands for Rest, Ice, Compression, and Elevation. For acute inflammation in the foot or ankle, your foot and ankle surgeon will recommend "RICE" therapy.
Rest. Stay off of your foot as much as possible to prevent further injury. In some cases, complete immobilization may be required. Your doctor will decide whether you will need
crutches and whether movement of your foot or ankle is appropriate.
Ice. Icing, which decreases blood flow to the tissue, thus reducing swelling and pain, should be continued until your symptoms resolve. Wrap ice cubes—or a bag of frozen peas or corn—in a thin towel and place the pack on the injured area for 20 minutes of each hour you’re awake. If your skin turns blue or white, discontinue icing for a few hours. Two cautions: Never apply ice or frozen bags directly to your skin. And never leave an ice pack on your injury while you sleep.
Compression. Keep the inflamed area compressed by wrapping it in an elastic bandage or stocking. Compression prevents additional fluid accumulation and helps reduce pain. Wrap the bandage more firmly at the toes and less firmly at the calf. If your toes tingle or your foot throbs, the wrapping may need to be loosened. If the tingling or throbbing continues after loosening the wrap, contact your doctor as soon as possible.
Elevation. Keeping the foot elevated reduces the swelling by allowing excess fluid to drain to the heart. The proper way to elevate your foot is to keep it level with or slightly above the heart. Place one or two pillows under your calf, and make sure your hip and knee are slightly bent. Never keep your leg extended straight out.


{kind=link}
{kind=link}